– Symptoms, Causes & Treatment")
A rare progressive neurological disorder, corticobasal syndrome (CBS) is a condition that causes changes in language skills, movement, or both.
What is Corticobasal Syndrome?
It is one of the illnesses that has caught the attention of behavioral neurologists and movement disorder specialists.
Also known as CBD (corticobasal degeneration) it may start with issues such as stiff muscles on one side of the body involving a leg, arm, or both.
Such motor abnormalities include apraxia which is the inability to perform voluntary or purposeful movements and muscle rigidity.
Persons with this condition often complain about having trouble controlling their arms or legs.
Historically, CBD was recognized as a neurological condition that was mostly associated with movement disorders.
However, in recent years, research has revealed that behavioral and cognitive abnormalities occur more often than what was believed.
In some cases, dementia warning signs may precede the development of motor symptoms.
The initial cognitive symptoms may include impairments in executive function, progressive aphasia, and loss of intellectual abilities.
CBS was first described in 1968 by Rebeiz and colleagues. Most people will this condition will start showcasing symptoms around the age of 60 but some will have the warning signs earlier.
What Causes Corticobasal Syndrome

Scientists are yet to identify the exact cause of CBS.
Experts, however, know that in some individuals with the condition, there is usually a large build-up of tau.
This is a type of protein that usually occurs in the brain, but it is not clear why it at times builds-up in large amounts.
The function of tau within the nerve cells is quite complex and experts do not fully understand it.
It is, however, thought that tau is essential for the normal functioning of brain cells.
The abnormal tau levels in various brain cells result in their deterioration. The specific role that tau plays in the development of corticobasal syndrome is not yet clear.
Tau abnormalities are observed in numerous neurodegenerative brain disorders like Pick’s disease, Alzheimer’s disease, frontotemporal dementia with parkinsonism linked to chromosome 17 (FTDP-17), Niemann-Pick disease type C, and progressive supranuclear palsy.
Collectively, these disorders are known as “tauopathies.”
Large build-up of amyloid plaques
Some people with CBS also have a large build-up of amyloid plaques which are similar to those present in individuals who have Alzheimer’s disease (AD).
The excessive accumulation of these proteins in the nerve cells is quite dangerous because it results in brain cells losing their ability to function normally, and they die off eventually.
As a result, the affected sections of the brain will start to shrink.
Researchers believe that several factors contribute to the development of CBD.
These include a combination of multiple environmental, genetic, and factors that relate to aging.
A person develops corticobasal degeneration symptoms due to the progressive deterioration of tissue in various areas of the brain.
The loss of nerve cells happens in specific areas resulting in shrinkage or atrophy in specific brain lobes.
The type and severity of symptoms that a person will get will depend on the section of the brain that has been affected by the condition.
Moreover, the 2 areas of the brain that are mostly affected include basal ganglia and cerebral cortex, but some other areas may also be affected.
The cerebral cortex is mostly involved with higher functions of the brain including learning, memory, voluntary movement, and sensory information coordination.
The basal ganglia can be described as a cluster of nerve cells that is responsible for learning and motor functions.
Symptoms of Corticobasal Syndrome
Trouble with movement is normally the first warning sign of CBS.
It may include poor coordination or trouble accomplishing simple goal-oriented activities like buttoning a shirt, gesturing with hands, or combing hair amongst others.
This symptom may start with one leg, arm, or hand. The limbs might shake and feel stiff.
Persons with this condition may experience movement that is slower than usual, go through changes in the feelings of the limbs or have a hard time making their limbs move.
As time goes by, moving around becomes harder.
In most cases, the symptoms will start on one side of the body and slowly move to the other side.
Other symptoms
Additional symptoms might include a slight tremor when a person is in a particular position or while performing a certain task.
Limb dystonia may also occur sometimes.
Dystonia describes a group of neurological conditions that are characterized by involuntary muscle contractions.
These put certain parts of the body into abnormal and sometimes painful positions and movements.
Affected persons may also experience contractures which is a condition where a joint becomes permanently fixed in an extended or bent position.
This can partially or completely restrict the movement of the joint that has been affected.
Alien limb phenomenon is also common in persons with CBS where a limb will carry out actions or assume certain positions without the awareness of the affected person.
Some individuals will also go through jerky or lightning-like movements.
Communication can become difficult
Language problems may also start to develop as the disease progresses.
Individuals may have challenges naming people and objects, finding the right words to speak, or just getting the words out mostly because of the problems with the muscles that help with speech.
After some time, people with malady may not be in a position to communicate effectively. Reading skills may start to diminish while writing can become harder especially if the movement symptoms have affected the hands.
Some people with CBD may also suffer problems with swallowing, uncoordinated walk, or inability to control eyelid blinking.
Others with CBS may also experience visuospatial difficulties or challenges seeing things and understanding their right place in space.
Persons with these challenges will have a difficult time locating things in space, grasping complex visual arrays like a cupboard, and judging distances while driving.
Individuals with the condition may also have a hard time with number knowledge and calculations.
It is also common for persons with CBS to develop memory problems where they keep repeating questions or misplace objects.
Later in the course of the illness, persons may experience personality changes.
This is where persons may exhibit disinhibition, reduced attention span, irritability, apathy, and obsessive-compulsive behaviors.
Some even get into the habit of saying inappropriate things. Others will experience difficulties when trying to move or open their eyes.
Eventually, persons with CBS might become bed-ridden and they may be susceptible to life-threatening complications like bacterial infections, pneumonia, blood infections, or blockage of one or more main arteries to the lungs primarily because of blood clots.
Keep in mind that the progression, severity, presentation, and symptoms of this disease vary greatly from one person to another.
Diagnosis

A positive diagnosis for corticobasal degeneration is suspected when characteristic neurologic warning signs occur progressively in the absence of a structural lesion like a tumor or stroke.
It is normally challenging to distinguish corticobasal degeneration from other related neurodegenerative disorders.
Currently, there are no tests for CBS.
A clinical diagnosis is done based on the pattern of symptoms and extensive neurological exam involving multiple specialized tests and these include:
An EEG (electroencephalogram)
This is a test that measures the brain’s electrical activity.
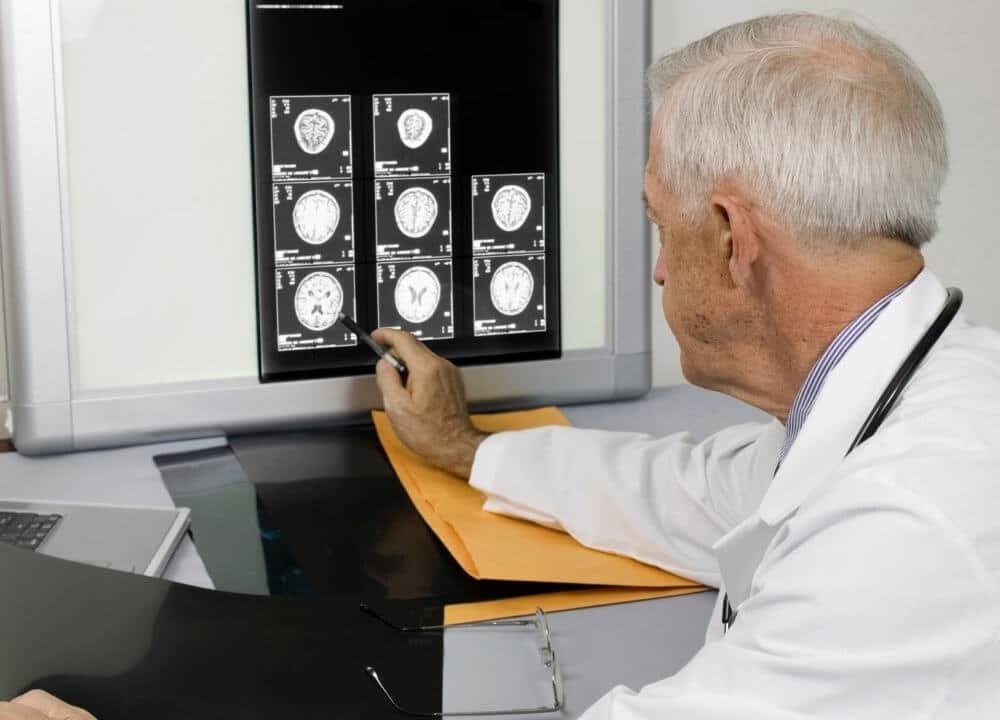
Imaging Techniques
CT (computerized tomography) and MRI ( magnetic resonance imaging) are helpful when it comes to ruling out other medical conditions. They also come in handy when the doctor wants to view brain tissue degeneration within the basal ganglia and cerebral cortex.
DaTscan
This technique measure the amount of dopamine which is a chemical that the brain makes.
Neuropsychological testing
It is where professionals conduct various memory tests with pictures and words. These are exclusive to evaluate the extent of a person’s symptoms and the impact they have on mental abilities.
The tests look into multiple abilities like concentration, numbers, counting, memory, understanding language, and how a person processes vital details such as words and pictures.
Diagnosis is also done to rule out other medical conditions that can cause similar symptoms like Alzheimer’s disease, motor neuron disease, and Parkinson’s disease.
It is important that a consultant with expertise in corticobasal degeneration confirms the diagnosis.
Most of the time, this will be a neurologist who is an expert in conditions that affect the nerves and brain.
In the majority of cases, the confirmation of the diagnosis is only possible once professionals conduct autopsy examinations of the brain.
This shows “ballooned” protein, neurons aggregations, and other characteristic abnormalities that are as a result of an abnormal build-up of tau protein.
Treatment Options

There is still no approved cure for the corticobasal syndrome. Nonetheless, there are several treatments that can benefit persons with the disease, and these include:
Medications
Doctors can prescribe medication that can help manage the symptoms. Examples of these drugs include cholinesterase inhibitors which are helpful if a person with CBS is having memory problems.
The most common medicines that persons take include rivastigmine, donepezil, and galantamine.
For the movement symptoms, an individual may be treated with drugs that are used for persons with Parkinson’s disease.
These include carbidopa or levodopa but the effects of the drugs are subject to research.
Physicians may also recommend drugs to help deal with other issues like incontinence and bladder problems, sleeping problems, anxiety, pain, and bone strength.
It is also important for physicians to treat any existing conditions that affect the brain.
These include high cholesterol, high blood pressure, and diabetes.
Eating Right and Working Out
Research indicates that getting physically active helps to improve brain health, general fitness, and mood.
Getting enough sleep, eating a balanced diet, and limiting alcohol intake also helps to promote good health.
Alternative Therapies
Several therapies can help people with CBS and these include:
Speech and Language Therapy
It can help enhance communication between people with the condition and others. The experts can also help manage swallowing problems.
Physical Therapy
This in addition to stretching exercises can help ease movement challenges by maintaining the range of motion and mobility of rigid stiffened joints as well as preventing the development of contractures.
Occupational Therapy
It may be useful in assessing the safety of an affected individual’s home as well as determining the adaptive medical equipment that may boost a person’s independence. That’s when occupational therapy comes into play. Affected people may need to use devices like a walker or a crane to assist in walking.
Cognitive Stimulation
This comes in handy for persons with CBS but is showcasing dementia symptoms. This type of therapy involves engaging in exercises and activities that aim to enhance language ability, problem-solving skills, and memory.
Palliative Care and Advanced Care Planning
Palliative care is normally offered to relieve pain as well as other distressing symptoms a person may be facing while offering spiritual, social, and psychological support.
This can be beneficial at any stage of CBD alongside other treatments. An individual can receive this type of care at home, in a hospital, or at a hospice.
Advanced care planning is where persons with the corticobasal syndrome will make plans for the future highlighting their wishes in regards to medical care and other important decisions.
Affected individuals share the plans with their family members and health professionals who are taking care of them.
Seeing that this is quite a rare condition, clinical trials may at times not be available for persons seeking them.
CBS Prognosis

Corticobasal degeneration is a condition that changes over time and is believed to affect females and males equally.
An individual with the disease can live for years after a positive diagnosis. Symptoms of the conditions tend to worsen over 3-8 years and often cause great disability.
Research suggests that a majority of affected individuals live for about 6-8 years on average although this varies from one person to the next.
Closing Thoughts
Even though currently there are no therapies or treatments that can reverse or slow down the progression of corticobasal syndrome, there is still hope.
Scientists reckon that the biology of CBS may be similar to that of other neurodegenerative diseases.
It is possible that therapies that are useful for these conditions can be helpful to persons with corticobasal degeneration.